
 |
Thursday, December 20, 2018
Wednesday, December 19, 2018
Surgeon General releases advisory on E-cigarette epidemic among youth
U.S. Surgeon General Vice Adm. Jerome M. Adams issued an advisory today stressing the importance of protecting children from a lifetime of nicotine addiction and associated health risks by immediately addressing the epidemic of youth e-cigarette use.
Data from National Institutes of Health’s Monitoring the Future survey also shows that America’s teens reported a dramatic increase in their use of e-cigarettes in just a single year, with 37.3 percent of 12th graders reporting use in the past 12 months, compared to 27.8 percent in 2017.
“We need to protect our kids from all tobacco products, including all shapes and sizes of e-cigarettes,” said Adams. “Everyone can play an important role in protecting our nation’s young people from the risks of e-cigarettes.”
The surge in e-cigarette use among our nation’s youth has been fueled by newer cartridge-based devices that have become increasingly popular. Many of these e-cigarettes look like a USB flash drive, making them easy to conceal. One of the most commonly sold versions is JUUL, which now has more than a 70 percent share of the cartridge-based e-cigarette market in the United States. A typical JUUL cartridge, or “pod,” contains about as much nicotine as a pack of 20 regular cigarettes.
“In the data sets we use, we have never seen use of any substance by America’s young people rise as rapidly as e-cigarette use is rising,” said HHS Secretary Alex Azar. “Combustible cigarettes remain the leading cause of preventable death in the United States, and providing an effective off-ramp for adults who want to quit using them is a public health priority. But we cannot allow e-cigarettes to become an on-ramp to nicotine addiction for younger Americans. HHS has been and will continue developing a comprehensive, balanced policy approach to this challenge.”
As noted in the 2016 Surgeon General’s report on E-cigarette Use Among Youth and Young Adults, e-cigarette use poses a significant – and avoidable – health risk to young people. Besides increasing the possibility of addiction and long-term harm to brain development and respiratory health, e-cigarette use may also lead to the use of regular cigarettes that can do even more damage to the body.
“We have evidence-based strategies to prevent tobacco use that can be applied to e-cigarettes.” said Adams. “We must take action now to protect the health of our nation’s young people.”
For facts about the risk of e-cigarettes, and how to protect our youth, visit: e-cigarettes.surgeongeneral.gov.
###
HHS recommends prescribing or co-prescribing naloxone to patients at high risk for an opioid overdose
HHS recommends prescribing or co-prescribing naloxone to patients at high risk for an opioid overdose
|
 Adm. Brett P. Giroir, MD, assistant secretary for health and senior advisor for opioid policy, today released guidance for healthcare providers and patients detailing how naloxone – the opioid overdose reversal drug – can help save lives and should be prescribed to all patients at risk for opioid complications, including overdose. Adm. Brett P. Giroir, MD, assistant secretary for health and senior advisor for opioid policy, today released guidance for healthcare providers and patients detailing how naloxone – the opioid overdose reversal drug – can help save lives and should be prescribed to all patients at risk for opioid complications, including overdose.“Given the scope of the opioid crisis, it’s critically important that healthcare providers and patients discuss the risks of opioids and how naloxone should be used in the event of an overdose,” said Adm. Giroir. “We have begun to see some encouraging signs in our response to the opioid crisis, but we know that more work is required to fully reverse the decades-long epidemic. Co-prescribing naloxone when a patient is considered to be at high risk of an overdose, is an essential element of our national effort to reduce overdose deaths and should be practiced widely.” To reduce the risk of overdose deaths, the guidance released today reinforces and expands upon prior CDC guidelines. It recommends that clinicians prescribe or co-prescribe (prescribed in conjunction with additional medication) naloxone to individuals at risk for opioid overdose, including, but not limited to: individuals who are on relatively high doses of opioids, take other medications which enhance opioid complications or have underlying health conditions. By co-prescribing, or prescribing naloxone to at risk individuals, patients and their loved ones could be better equipped for a possible complications of overdose, including slowed or stopped breathing. Clinicians should also educate patients and those who are likely to respond to an overdose, including family members and friends, on when and how to use naloxone in its variety of forms. Naloxone is an FDA-approved medication that can save a person’s life when administered during an opioid overdose. Naloxone reverses the effects of opioids, such as stopped or slowed breathing. However, for naloxone to revive individuals who have experienced an opioid overdose, it must be in the right hands at the right time and administered within minutes of life-threatening symptoms. Naloxone is available in a variety of forms (nasal spray, injection, auto-injector); and at least one form is covered by most health insurance plans, including Medicaid and Medicare. “Promoting the targeted availability and distribution of overdose-reversing drugs is one of the five pillars of HHS’s comprehensive, science-based strategy for the opioid epidemic,” said Health and Human Services Secretary Alex Azar. “This new guidance reflects our commitment to ensuring those who need overdose-reversing drugs have them and provides practical steps that clinicians, patients, and the public can take to reduce the risk of an overdose.” In April 2017, HHS announced its 5-Point Strategy to Combat the Opioids Crisis. Those efforts include: better addiction prevention, treatment, and recovery services; better data; better pain management; better targeting of overdose reversing drugs; and better research. In April 2018, Surgeon General VADM Jerome Adams issued an unprecedented advisoryencouraging more individuals, including family, friends, and those who are personally at risk for an opioid overdose to carry naloxone. Today’s guidance will bolster HHS’ ongoing efforts to combat the opioid crisis and expand the use of naloxone. To view the guidance, click here. To learn more about HHS’s efforts to combat the opioid crisis, visit www.hhs.gov/opioids. |
###
|
Friday, December 14, 2018

Thursday, December 13, 2018
2019 Open Enrollment is here – and ends Dec 15
You can enroll in or change 2019 Marketplace health insurance right now. The 2019 Open Enrollment Period runs from Thursday, November 1, 2018, to Saturday, December 15, 2018.
 IMPORTANT: 2019 Open Enrollment ends December 15
IMPORTANT: 2019 Open Enrollment ends December 15
If you don’t act by December 15, you can’t get 2019 coverage unless you qualify for a Special Enrollment Period. Plans sold during Open Enrollment start January 1, 2019.
If you don’t act by December 15, you can’t get 2019 coverage unless you qualify for a Special Enrollment Period. Plans sold during Open Enrollment start January 1, 2019.
Wednesday, December 12, 2018
Action for Dental Health Act signed into law

Today, President Trump signed into law the Action for Dental Health Act, a bipartisan bill aimed at improving oral health and access to oral health care.
H.R. 2422, introduced by Reps. Robin Kelly (D-IL) and Mike Simpson (R-ID) passed the House in February; in October, it passed the Senate, where it was sponsored by Sens. Cory Booker (D-NJ) Bill Cassidy (R-LA) Mazie Hirono (D-HI), and Tim Scott (R-SC).
The Action for Dental Health Act amends the Public Health Service Act to reauthorize oral health promotion and disease prevention programs through FY2022. Significantly, it expands eligibility of the types of organizations able to apply for Health and Human Services (HHS) grants to improve oral health through education and dental disease prevention. The grants will also be used to develop and expand outreach programs, establish dental homes for children and adults, including the elderly, blind and disabled and facilitate the provision of dental care to nursing home residents.
“This legislation is encouraging and signals oral health is a priority of Congress. Increasing oral health education and preventive oral health programs will be key to improving early diagnosis, intervention and prevention programs for our communities,” says Beth Truett, President and CEO of Oral Health America, “OHA is eager to work alongside its partners and members of Congress to improve oral health outcomes for all.”
New Youth Risk Behavior Surveillance System Analysis Tool Released
Today, the Division of Adolescent and School Health (DASH) released a Youth Risk Behavior Surveillance System (YRBSS) Analysis Tool as an enhancement to the Youth Online data analysis tool that provides users with easy access to data on health-risk behaviors that contribute to the leading causes of death and disability among youth and adults. The YRBSS Analysis Tool can be accessed through Youth Online which can be found on the Youth Risk Behavior Survey (YRBS) website at www.cdc.gov/healthyyouth/data/
The release includes:
A New YRBSS Analysis Tool that allows users to explore YRBSS and Global School-based Student Health Survey (GSHS) data in more detail by conducting cross tabulation analyses that compare data for two variables, with the option of stratifying the results by year, site, demographic variables or sexual orientation.
Youth Online Background:
Youth Online allows users to analyze national, state, and local YRBSS data from high school and middle school surveys conducted during 1991-2017 and GSHS data from students aged 13-17 conducted during 2003-2015. YRBSS data can be filtered and sorted on the basis of race/ethnicity, sex, academic grade, and sexual orientation while GSHS data can be filtered and sorted on sex and age. Additionally you can filter and sort both surveys by location and year, create customized tables, maps, graphs, and perform statistical tests by location and health topic.
For more information about YRBS:
- Web site: www.cdc.gov/healthyyouth/data/
yrbs - Phone: 1-800-CDC-INFO (1-800-232-4636)
- Email: nccddashinfo@cdc.gov
Tuesday, December 11, 2018
Healthy People public comment period open until January 17, 2019

The U.S. Department of Health and Human Services (HHS) is soliciting written comments on the proposed objectives for Healthy People 2030. This public comment period will allow comments on the proposed HP2030 objectives and members of the public can also propose their own objectives.
Previous public comments on the proposed Healthy People 2030 framework helped shape the vision, mission, foundational principles, plan of action, and overarching goals for Healthy People 2030. In this public comment period, HHS would like input on the proposed Core, Developmental, and Research objectives.
In response to stakeholder input, Healthy People 2030 will be a streamlined set of national health objectives guiding the Nation in efforts to improve health. Healthy People 2030 will continue to represent critical public health priorities by addressing the leading causes of morbidity and mortality and driving action at the national, state, and local levels.
Members of the public are invited to submit comments on the proposed objectives from December 3, 2018, to January 17, 2019. Learn more and submit your comments today!
Tuesday, December 4, 2018
The Utah Health Improvement Index: A New Tool to Advance Health Equity

Developed by the Utah Department of Health (UDOH), the Utah Health Improvement Index (HII) is a measure of health equity. It includes nine indicators that describe important aspects of demographics, socioeconomic deprivation, economic inequality, resource availability, and opportunity structure.
Those indicators are:
• Population aged ≥25 years with <9 years of education, %
• Population aged ≥25 years with at least a high school diploma, %
• Median family income, $
• Income disparity
• Owner-occupied housing units, % (home ownership rate)
• Civilian labor force population aged ≥16 years unemployed, % (unemployment rate)
• Families below poverty level, %
• Population below 150% of the poverty threshold, %
• Single-parent households with children aged <18 years, %
The HII is based on Utah Small Areas (geographic areas based on ZIP codes, local health districts, county boundaries, and input from local community representatives). The new small areas were released by UDOH in October 2018. There are 99 small areas in Utah.
The 99 small areas are categorized into five groups: very low (20 areas), low (25), average (18), high (20), and very high (16) health improvement areas. The HII ranks from 71.89 to 160.87. The higher the ranking, the more improvements the area needs.
This classification can be used as a guide to determine the type of intervention to implement in order to advance health equity and reduce, in an efficient and effective way, the burden of diseases and health conditions in specific geographic areas.
The HII is the result of a collaboration project between the Office of Health Disparities and the Bureau of Health Promotion. More information about the HII and its practical applications will be available soon.
Monday, December 3, 2018

Utah's Office of Health Disparities at APHA

 The Utah Department of Health Office of Health Disparities (OHD) was chosen among many applicants to present at this year's American Public Health Association (APHA) Annual Meeting & Expo about the It Takes A Village Project. It Takes a Village is a community education and engagement series specifically designed for Utah's Native Hawaiian/Pacific Islander communities who are facing birth outcomes disparities.
The Utah Department of Health Office of Health Disparities (OHD) was chosen among many applicants to present at this year's American Public Health Association (APHA) Annual Meeting & Expo about the It Takes A Village Project. It Takes a Village is a community education and engagement series specifically designed for Utah's Native Hawaiian/Pacific Islander communities who are facing birth outcomes disparities.The presentation titled "It Takes a Village: Giving Our Babies the Best Chance" was offered by OHD's Brittney Okada, MPH, CHES on Wednesday, November 14. Participants were interested in learning about how OHD developed this unique curriculum and utilized specific cultural concepts to present key health concepts. Participants from around the country were also interested to learn how Utah disaggregates data and how large the NHPI community is here. Learn more about the ITAV project and view the curriculum.
Oral Health America Webinar Series: Oral care for infants and toddlers
 Inspiring and Innovative Preventive Oral Care for Infants and Toddlers
Inspiring and Innovative Preventive Oral Care for Infants and Toddlers Presenter: Hamida Askaryar MPH, RDH, MCHES
December 12, 2018 at 2:00 PM CST
This session will focus on minimally invasive preventive oral health care for infants and toddlers, the value of interprofessional medical/dental community partnerships, and the six-step care process including motivational interviewing to selecting self-management goals to achieve improved health outcomes.
Key points:
- Prevalence of early childhood caries and why we need to address it
- Early establishment of a dental home y 12 months- bio-behavioral model (“Age one visit”)
- Systemic-oral health link
- Medical-dental integration models
- Caries risk assessments using Caries Management by Risk Assessment (CAMBRA)- and risk-based combination therapies
- White spot lesions- what can providers and parents do?
To Register: https://attendee.
Friday, November 30, 2018
December 7: Improving Dementia Outcomes Among Underserved Populations

A full-fledged public health response is needed to improve outcomes in communities disproportionately impacted by Alzheimer’s and other dementias. Join the Society for Public Health Education’s webinar on Friday, December 7, 2018, from 12:30 to 1:30 pm ET — Healthy Brain Initiative: Improving Dementia Outcomes for African Americans and Asian American/Pacific Islander Populations. Please register in advance.
The new Healthy Brain Initiative (HBI) State and Local Public Health Partnerships to Address Dementia: The 2018-2023 Road Map has a central goal of reducing disparities among underserved populations. The HBI Road Map’s quick-start guide has 25 actions to promote brain health, increase early detection, enhance safety and quality of care, and support caregivers’ health and effectiveness. Webinar participants will learn about health education and health promotion initiatives that implement Road Map actions and aim to improve outcomes among African Americans, Asian Americans and Pacific Islanders, and American Indians/Alaska Natives (AI/AN).
Presenters include Molly French, Director of Public Health for the Alzheimer’s Association, Dr. Lisa McGuire, Lead of the Alzheimer’s Disease and Healthy Aging Program for the Centers for Disease Control and Prevention (CDC), and Marci Getz, Senior Health Educator for the Washington State Department of Health.
Presenters include Molly French, Director of Public Health for the Alzheimer’s Association, Dr. Lisa McGuire, Lead of the Alzheimer’s Disease and Healthy Aging Program for the Centers for Disease Control and Prevention (CDC), and Marci Getz, Senior Health Educator for the Washington State Department of Health.
Please be sure to register in advance and mark your calendars for this interactive webinar.
Thursday, November 29, 2018
How long can we expect to live?
Data from the National Vital Statistics System
The CDC National Center for Health Statistics released the Mortality in the United States; 2017 report.
- Life expectancy for the U.S. population declined to 78.6 years in 2017.
- The age-adjusted death rate increased by 0.4% from 728.8 deaths per 100,000 standard population in 2016 to 731.9 in 2017.
- Age-specific death rates increased from 2016 to 2017 for age groups 25–34, 35–44, and 85 and over, and decreased for the age group 45–54.
- The 10 leading causes of death in 2017 remained the same as in 2016.
- The infant mortality rate of 579.3 infant deaths per 100,000 live births in 2017 was not significantly different from the 2016 rate.
- The 10 leading causes of infant death in 2017 remained the same as in 2016 although 4 causes changed ranks.
Figure 1. Life expectancy at selected ages, by sex: United States, 2016 and 2017
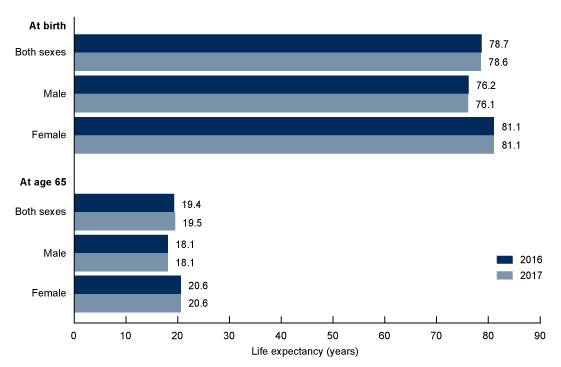
NOTES: Life expectancies for 2016 were revised using updated Medicare data; therefore, figures may differ from those previously published. Access data table for Figure 1
SOURCE: NCHS, National Vital Statistics System, Mortality.
SOURCE: NCHS, National Vital Statistics System, Mortality.
Wednesday, November 28, 2018
Privacy and Confidentiality Protections: issues surrounding the Opioid Crisis webinar Nov 29
Thursday, November 29, 1 – 230 MT: Privacy and Confidentiality Protections: Substance Use Disorders and the Opioid Crisis. The next call from the Region VIII Opioid Misuse Consultation Team will include speakers from the Office for Civil Rights and from the Substance Abuse and Mental Health Services Administration and will focus on HIPAA and 42 CFR as applied to substance use treatment issues. Pre-registration is not required.
When it's time, join the meeting from here:
Join the meeting
Access Information: To join the audio portion of the meeting
1. Please call the following number: WebEx: 1-877-267-1577
2. Follow the instructions you hear on the phone. Your WebEx Meeting Number: 992 545 720
To view this meeting:
1. Go to https://meetings.cms.gov/orion/joinmeeting.do?MTID=0236d05c02294bf1331b5a83b9ea1aeb
2. If requested, enter your name and email address.
3. If a password is required, enter the meeting password: (This meeting does not require a password.)
4. Click "Join".
5. Follow the instructions that appear on your screen.
AGENDA (all times mountain)
1:00 – 1:05 pm: Welcome and housekeeping (Christina Mead or Charlie Smith)
1:05 – 1:30 pm: HIPAA PRIVACY RULE: OCR will provide an overview of how the HIPAA Privacy Rule protects information regarding substance use and abuse and how it allows for information sharing that is necessary to aid in treatment. Specifically, OCR will discuss the access provisions of the Privacy Rule, as well as OCR’s guidance related to opioid overdose and sharing information related to mental health.
1:30-1:55 pm: 42 CFR Part 2: Confidentiality of Substance Use Disorder Patient Records is a Federal law that protects and ensures the rights of patients receiving treatment for a Substance Use Disorder (SUD) so that they do not face adverse consequences as a result of their SUD treatment such as arrest, child custody, divorce or employment proceedings. This presentation will briefly review the components of 42 CFR Part 2 and considerations relative to community and provider responses to the opioid epidemic.
1:55-2:15 pm: State and Federal Leadership comments and announcements
2:15-2:30 pm: Discussion and Q&A
2:30 pm: Adjourn
When it's time, join the meeting from here:
Join the meeting
Access Information: To join the audio portion of the meeting
1. Please call the following number: WebEx: 1-877-267-1577
2. Follow the instructions you hear on the phone. Your WebEx Meeting Number: 992 545 720
To view this meeting:
1. Go to https://meetings.cms.gov/orion/joinmeeting.do?MTID=0236d05c02294bf1331b5a83b9ea1aeb
2. If requested, enter your name and email address.
3. If a password is required, enter the meeting password: (This meeting does not require a password.)
4. Click "Join".
5. Follow the instructions that appear on your screen.
AGENDA (all times mountain)
1:00 – 1:05 pm: Welcome and housekeeping (Christina Mead or Charlie Smith)
1:05 – 1:30 pm: HIPAA PRIVACY RULE: OCR will provide an overview of how the HIPAA Privacy Rule protects information regarding substance use and abuse and how it allows for information sharing that is necessary to aid in treatment. Specifically, OCR will discuss the access provisions of the Privacy Rule, as well as OCR’s guidance related to opioid overdose and sharing information related to mental health.
- Speaker: Emily Prehm, J.D., Equal Opportunity Specialist, U.S. Department of Health and Human Services Office for Civil Rights, Rocky Mountain Region. Emily Prehm is an Equal Opportunity Specialist with the U.S. Department of Health and Human Services, Office for Civil Rights (OCR), Rocky Mountain Region in Denver, Colorado. She began working with OCR in 2002 as a Legal Intern. Emily received a Juris Doctor degree from the University of Colorado at Boulder and is licensed to practice law in the state of Colorado.
1:30-1:55 pm: 42 CFR Part 2: Confidentiality of Substance Use Disorder Patient Records is a Federal law that protects and ensures the rights of patients receiving treatment for a Substance Use Disorder (SUD) so that they do not face adverse consequences as a result of their SUD treatment such as arrest, child custody, divorce or employment proceedings. This presentation will briefly review the components of 42 CFR Part 2 and considerations relative to community and provider responses to the opioid epidemic.
- Speaker: Charles H. Smith, Ph.D., Regional Administrator, Substance Abuse and Mental Health Services Administration (SAMHSA) U.S. Department of Health and Human Services – Region VIII (Colorado, Montana, North Dakota, South Dakota, Utah, and Wyoming). Dr. Smith is the Regional Administrator for the Substance Abuse and Mental Health Services Administration (SAMHSA), U.S. Department of Health and Human Services - Region VIII. Dr. Smith is the former Director of the Colorado Division of Behavioral Health and Deputy Commissioner of Mental Health and Substance Abuse for the State of Colorado. Dr. Smith is a Licensed Psychologist with over 25 years of experience in fields of forensic psychology, addictions, suicide prevention, crisis intervention, behavioral health policy and administration.
1:55-2:15 pm: State and Federal Leadership comments and announcements
2:15-2:30 pm: Discussion and Q&A
2:30 pm: Adjourn
SAMHSA FOA/Grant Opportunity Announcements
The Substance Abuse and Mental Health Services Administration (SAMHSA) released the following funding opportunity announcements (FOA). Below is information on the FOA’s as well as the link for additional information. Please share it with your colleagues and tribal stakeholders.
- Short Title: Healthy Transitions
- FOA Number: SM-19-001
- Application Due Date: Friday, December 21, 2018
- Purpose: The purpose of this program is to improve access to treatment and support services for youth and young adults, ages 16-25, who have a serious emotional disturbance or a serious mental illness, hereafter referred to as serious mental disorders.
- Eligibility: Federally recognized (as defined in Section 4[b] and Section 4[c] of the Indian Self-Determination Act) American Indian/Alaska Native (AI/AN) tribes, tribal organizations and consortia of tribes or tribal organizations. Note: Recipients who received funding under SM-18-010 Healthy Transitions are not eligible to apply for funding under this FOA. Recipients who received funding under SM-14-017 Now is the Time: Healthy Transitions are eligible to apply for funding under this FOA but must select two different communities with whom to partner with.
- Anticipated Total Available Funding: $14,130,226
- Anticipated Number of Awards: Up to 14 (At least 3 awards will be made to tribes/tribal organizations pending sufficient application volume from these groups).
- Anticipated Award Amount: $1,000,000 per year
- Length of Project: Up to 5 years
- Cost Sharing/Match Required?: No
- Short Title: SCN
- FOA Number: SM-19-002
- Application Due Date: Monday, December 24, 2018
- Purpose: The purpose of this program is to improve efforts to address the needs of adults with serious mental illness (SMI) by developing and/or expanding peer support services, peer leadership, and peer engagement strategies statewide.
- Eligibility: Eligibility is limited to domestic public and private non-profit entities, tribes, and Urban Indian organizations that are mental health consumer-operated organizations for at least two years and are not operating under the umbrella of another organization. Note: Recipients in states, tribes, or territories who received Statewide Consumer Network funding under SM-16-002 or SM-18-008 are not eligible to apply.
- Anticipated Total Available Funding: $883,876
- Anticipated Number of Awards: 9
- Anticipated Award Amount: Up to $95,000 per year
- Length of Project: Up to 3 years
- Cost Sharing/Match Required?: No
- Short Title: AWARE-SEA
- FOA Number: SM-19-003
- Application Due Date: Monday, December 24, 2018
- Purpose: The purpose of this program is to build or expand the capacity of State Educational Agencies, in partnership with State Mental Health Agencies overseeing school-aged youth and local education agencies.
- Eligibility: Education Agencies/Authorities serving children and youth residing in federally recognized American Indian/Alaska Native (AI/AN) tribes, tribal organizations, and consortia of tribes or tribal organizations.
- Anticipated Total Available Funding: $15,206,308
- Anticipated Number of Awards: 8 (At least 2 awards will be made to Tribal Education Agencies/Authorities pending sufficient application volume from these groups).
- Anticipated Award Amount: $1,800,000 per year
- Length of Project: Up to 5 years
- Cost Sharing/Match Required?: No
- Short Title: SFN
- FOA Number: SM-19-004
- Application Due Date: Friday, January 4, 2018
- Purpose: The purpose of this program is to better respond to the needs of children and adolescents with serious emotional disturbance and their families by providing information, referrals, and support; and to create a mechanism for families to participate in state and local mental health services planning and policy development.
- Eligibility: Eligibility is limited to family-controlled domestic public and private non-profit organizations in states, territories, and tribes. Note: Recipients in states and territories who received SFN funding under SM-18-007 are not eligible to apply.
- Anticipated Total Available Funding: $1,448,985
- Anticipated Number of Awards: 15 (At least 3 awards to family controlled organizations in tribes pending sufficient application volume from these groups).
- Anticipated Award Amount: Up to $95,000 per year
- Length of Project: Up to 3 years
- Cost Sharing/Match Required?: No
- Short Title: Native Connections
- FOA Number: SM-19-005
- Application Due Date: Friday, January 4, 2019
- Purpose: The purpose of this program is to prevent and reduce suicidal behavior and substance use, reduce the impact of trauma, and promote mental health among American Indian/Alaska Native youth through the age of 24 years.
- Eligibility: Eligibility is limited to federally recognized American Indian/Alaska Native tribes, tribal organizations, Urban Indian Organizations, or consortia of tribes and tribal organizations.
- Anticipated Total Available Funding: $12,797,090 (CMHS - $8,476,531; CSAP - $4,320,559)
- Anticipated Number of Awards: 51
- Anticipated Award Amount: Up to $250,000 per year
- Length of Project: Up to 5 years
- Cost Sharing/Match Required?: No
- Short Title: Family Treatment Drug Courts (FTDC)
- FOA Number: TI-19-001
- Application Due Date: Friday, January 4, 2019
- Purpose: The purpose of this grant program is to expand substance use disorder (SUD) treatment services in existing family treatment drug courts, which use the family treatment drug court model in order to provide alcohol and drug treatment to parents with an SUD and/or co-occurring SUD and mental health disorder who have had a dependency petition filed against them or are at risk of such filing.
- Eligibility: Eligibility is limited to federally recognized American Indian/Alaska Native tribes, tribal organizations, Urban Indian Organizations, or consortia of tribes and tribal organizations. Note: Family treatment drug courts that received an award under TI-17-004 (FY 2017 Grants to Expand Substance Abuse Treatment Capacity in Family Treatment Drug Courts) and TI-18-002 (FY 2018 Grants to Expand Substance Abuse Treatment Capacity in Family Treatment Drug Courts) are not eligible to apply for this funding opportunity.
- Anticipated Total Available Funding: $10,625,000
- Anticipated Number of Awards: 25 (At least 5 awards will made to tribes/tribal organizations pending sufficient application volume from these groups).
- Anticipated Award Amount: Up to $425,000 per year
- Length of Project: Up to 5 years
- Cost Sharing/Match Required?: No
- Short Title: SAMHSA Treatment Drug Courts (FTDC)
- FOA Number: TI-19-002
- Application Due Date: Friday, January 4, 2019
- Purpose: The purpose of this program is to expand substance use disorder (SUD) treatment services in existing adult problem solving courts, and adult Tribal Healing to Wellness courts, which use the treatment drug court model in order to provide SUD treatment (including recovery support services, screening, assessment, case management, and program coordination) to defendants/offenders.
- Eligibility: Eligibility is limited to federally recognized American Indian/Alaska Native tribes, tribal organizations, Urban Indian Organizations, or consortia of tribes and tribal organizations. Note: ATDCs and Adult Tribal Healing to Wellness Courts funded in FY2017 under announcement TI-17-001 and FY 2018 under announcement TI-18-008 are not eligible to apply for this program.
- Anticipated Total Available Funding: $10,000,000
- Anticipated Number of Awards: 25 (At least 5 awards will made to tribes/tribal organizations pending sufficient application volume from these groups).
- Anticipated Award Amount: Up to $400,000 per year
- Length of Project: Up to 5 years
- Cost Sharing/Match Required?: No
Monday, November 26, 2018
HRSA-led study estimates 1 in 40 U.S. children has diagnosed autism
| |||||||
Tuesday, November 20, 2018
The Opioid Crisis Symposium


Utah Law Review Symposium
The Opioid Crisis: Paths Forward to Mitigate Regulatory Failure
Friday, November 30, 2018
8:00 a.m. – 3:30 p.m., S.J. Quinney College of Law, Level 6
The 2018-2019 Utah Law Review presents “The Opioid Crisis: Paths Forward to Mitigate Regulatory Failure.” The symposium will critically examine failures of the pharmaceutical market, subsequent inadequate regulatory responses, and possible solutions as the nation moves forward in addressing the crisis. Scholars from around the country will discuss the impact of regulation from the national and state level, the impact of addiction on communities, and how public health research should inform future policy and regulation decisions. Read more »
The 2018-2019 Utah Law Review presents “The Opioid Crisis: Paths Forward to Mitigate Regulatory Failure.” The symposium will critically examine failures of the pharmaceutical market, subsequent inadequate regulatory responses, and possible solutions as the nation moves forward in addressing the crisis. Scholars from around the country will discuss the impact of regulation from the national and state level, the impact of addiction on communities, and how public health research should inform future policy and regulation decisions. Read more »
5 hours of CLE (pending). Lunch provided. Free and open to the public but registration is requested.
Panel discussions include:
- U.S. Food and Drug Administration
- The Public Health Perspective: Tracing the Root of the Problem
- The Role of States in Regulation
- The Community Impact of the Opioid Crisis: Addiction, Criminal Justice, and Health Disparities
Free parking is available at the Rice-Eccles Stadium. We encourage you to use public transportation to our events. Take TRAX University line to the Stadium stop and walk a half block north.
SOAR online training modules now available in Spanish
 SOAR Online is a new series of CE/CME training modules that you can complete whenever, wherever you like. Each module discusses the SOAR framework and how to apply it where you work to identify individuals who are at risk of trafficking or who have been trafficked—and connect them with the resources they need.
SOAR Online is a new series of CE/CME training modules that you can complete whenever, wherever you like. Each module discusses the SOAR framework and how to apply it where you work to identify individuals who are at risk of trafficking or who have been trafficked—and connect them with the resources they need.
The three training modules available now in Spanish include:
SOAR to Health and Wellness
Trauma-Informed Care
Culturally and Linguistically Appropriate Services
|
|
Subscribe to:
Posts (Atom)